Immediate Implants in the Esthetic Zone: When “Yes” Means Yes and When It Should Mean “Not Yet”
Immediate implant placement in the esthetic zone is still one of the most appealing treatment options we offer, but the literature keeps reminding us that success is driven less by speed than by case selection. In low-risk patients with an intact wall of buccal bone, immediate placement appears to provide similar esthetic and clinical outcomes—so the real question is not “Can we place it today?” but “Is this truly a low-risk socket?”
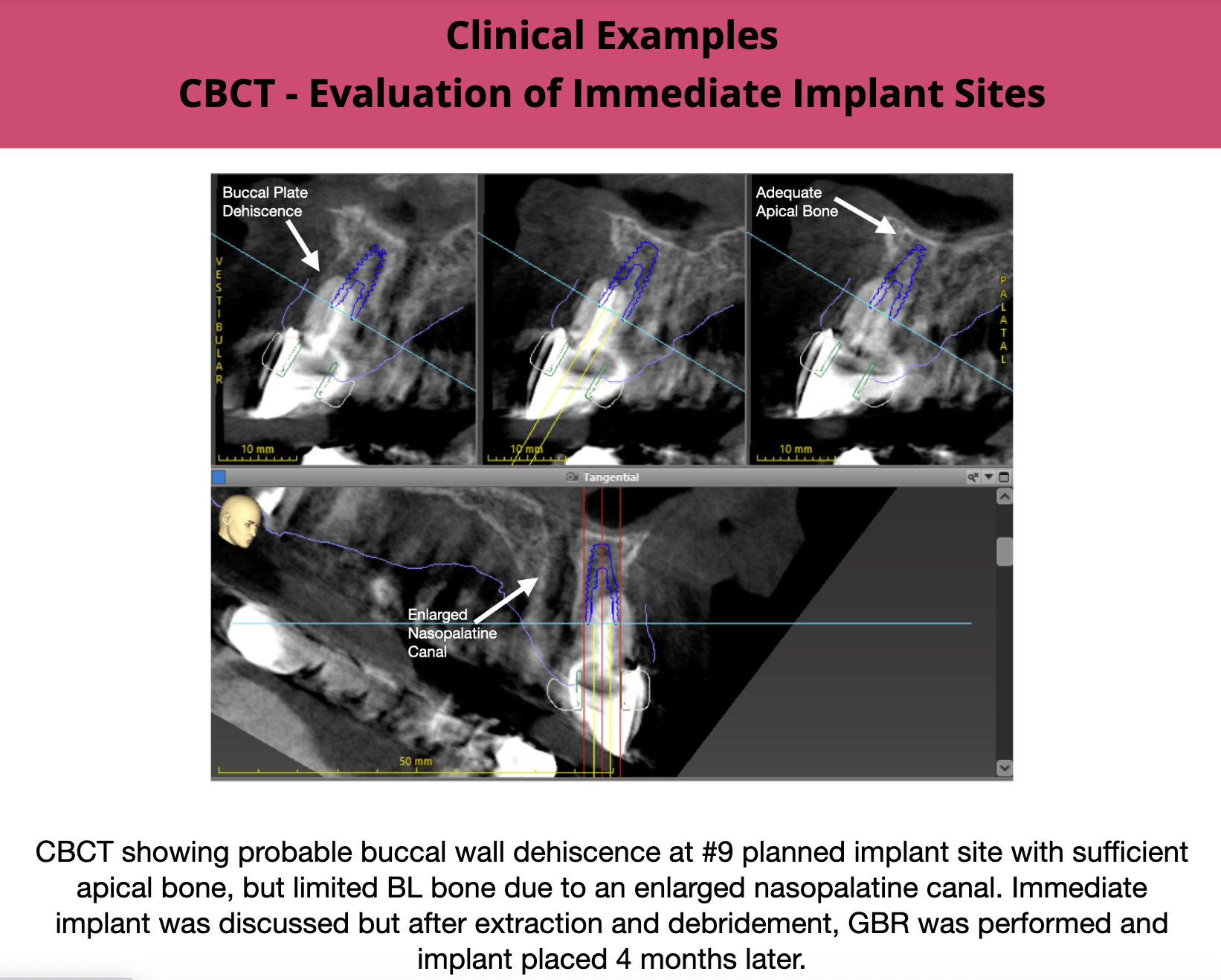
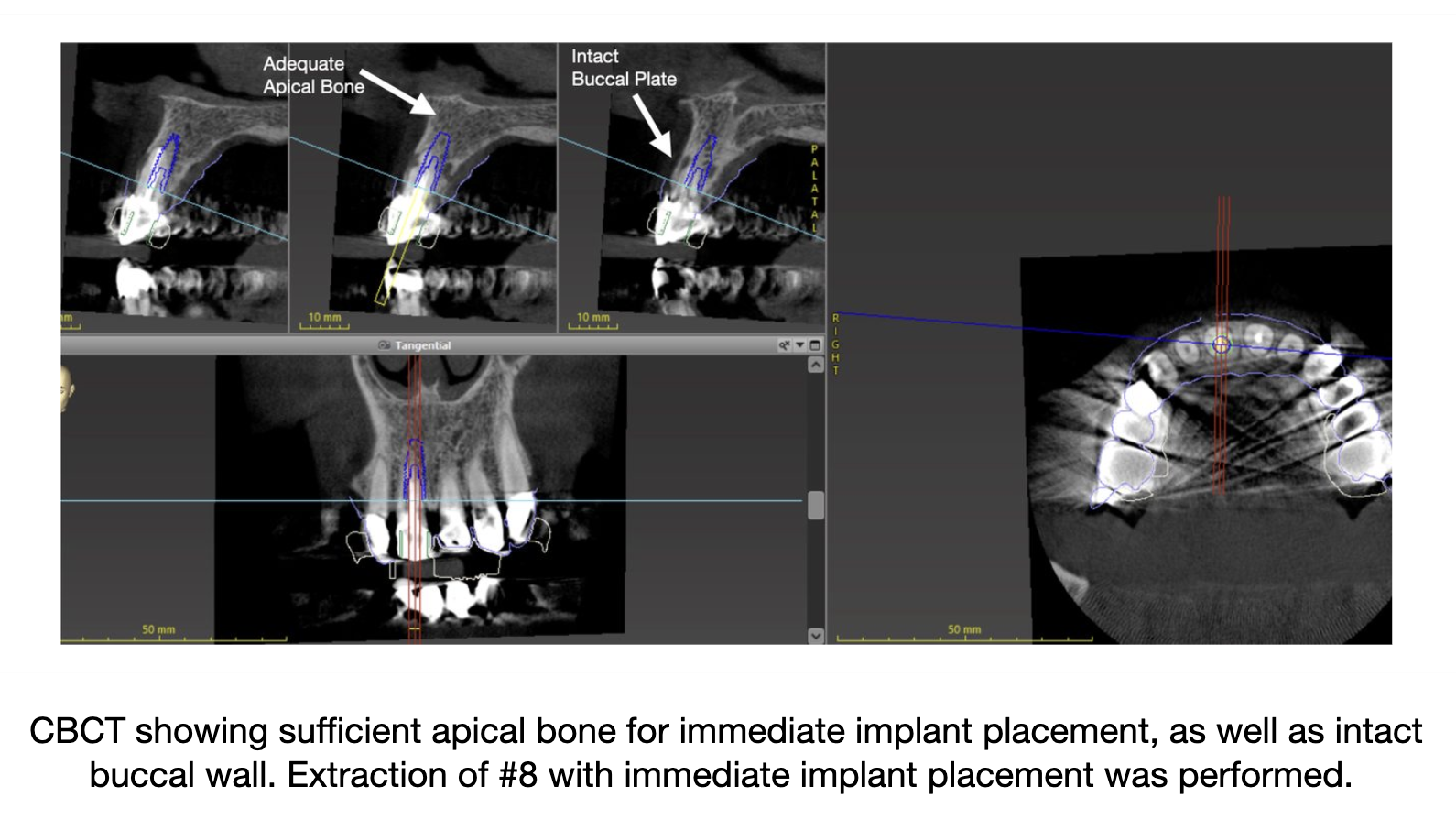
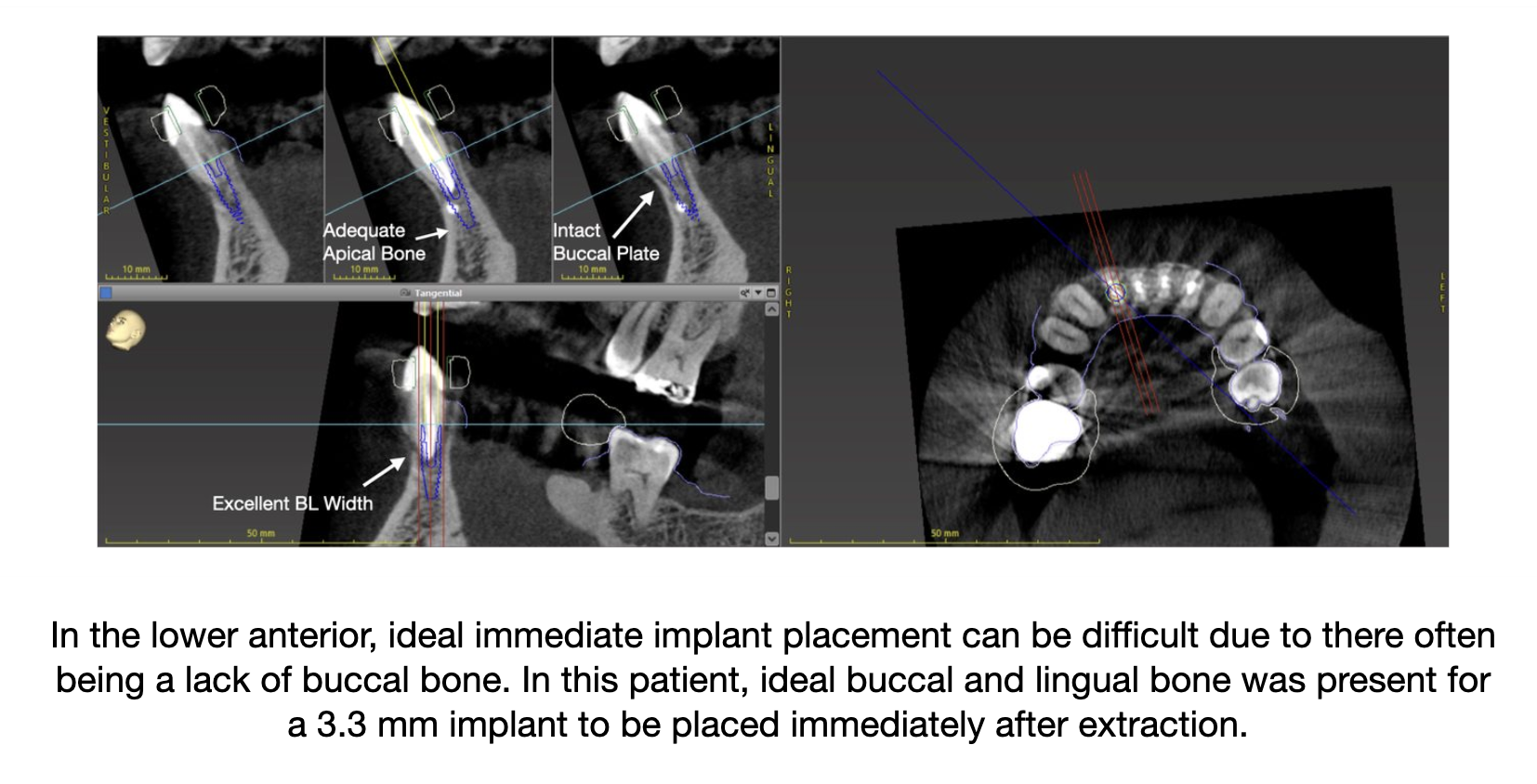
Our ideal immediate case is a failing single tooth with an intact facial/buccal wall (preferably at least 1 mm thick), a thick periodontal phenotype, minimal existing midfacial recession, and a prosthetically driven palatal implant position that preserves roughly 2 mm from the buccal wall. For maxillary central incisors, the CBCT also needs to confirm that the nasopalatine foramen will not force a compromised trajectory or leave inadequate bone anterior to the canal.
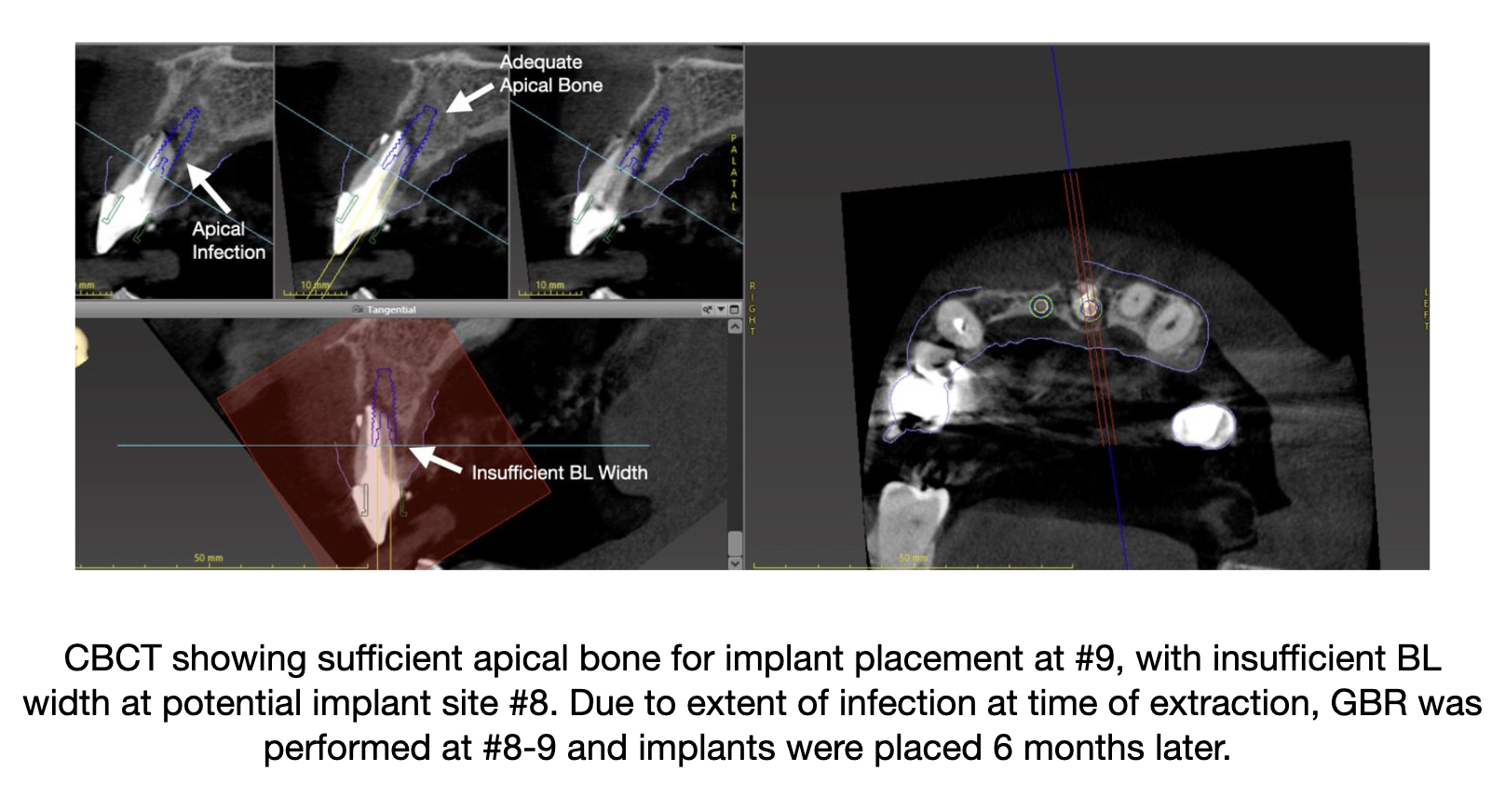
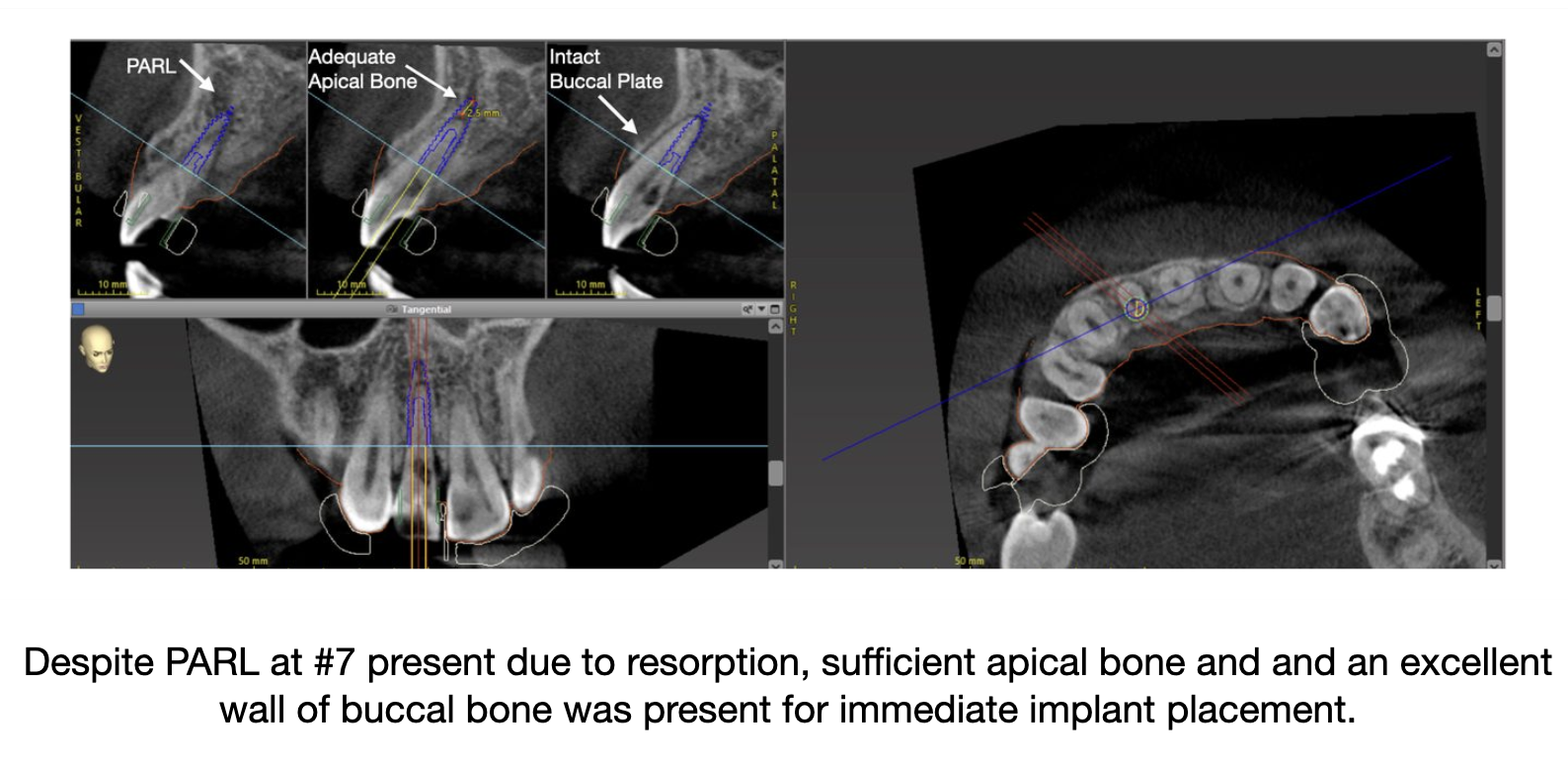
A PARL at the intended site is not an automatic “no.” Systematic reviews report that immediate implants in infected or periapical lesion sites can succeed when the lesion is chronic, the socket is meticulously debrided, and the facial wall remains favorable; however, the evidence is mixed, and we become much less enthusiastic when infection is acute or suppurative, when the lesion has already compromised the buccal bone, or when an adjacent tooth still carries untreated pulpal/periapical disease because of the risk of retrograde peri-implantitis.
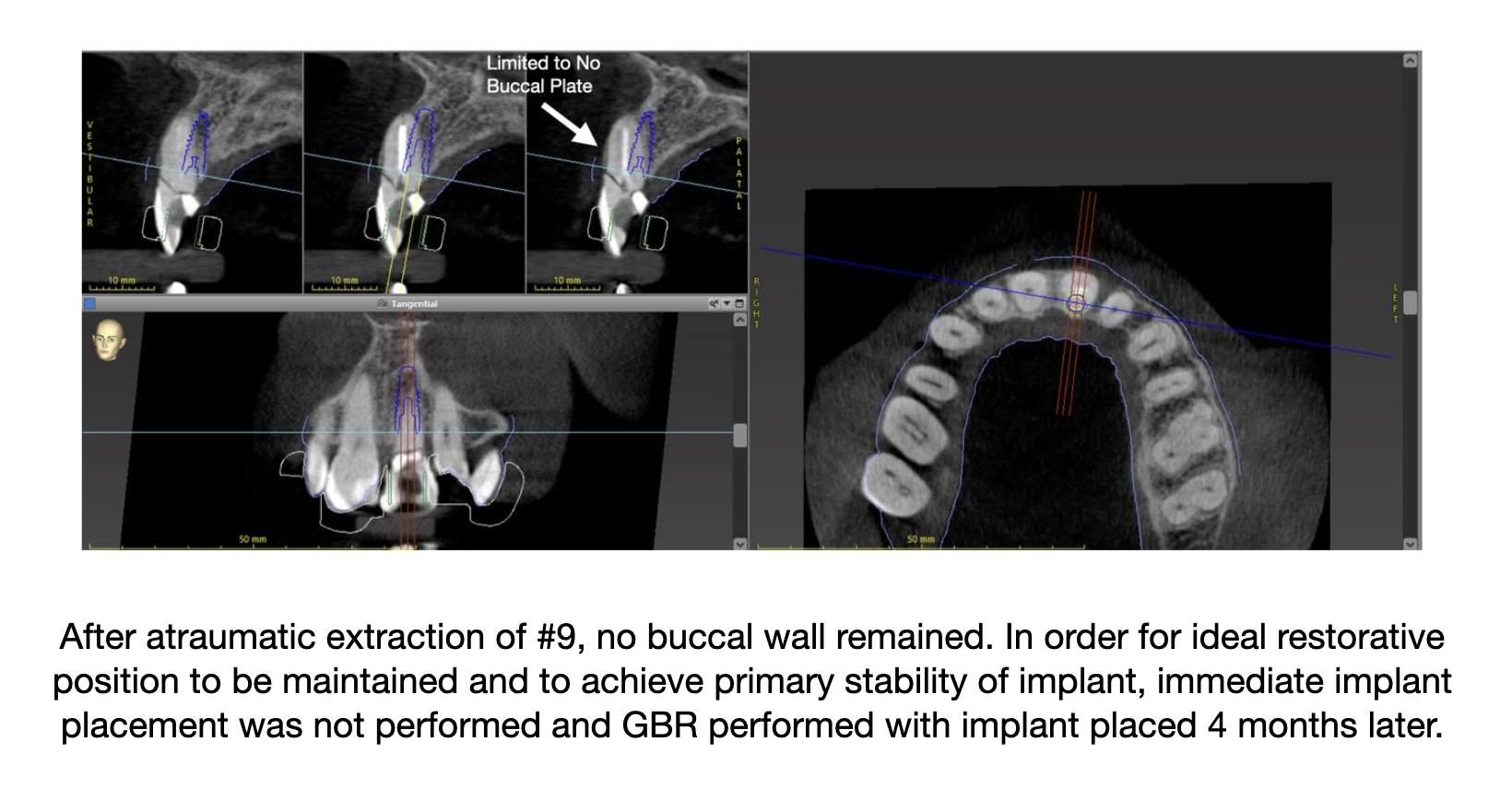
Our practical rule: immediate placement is possible and preferred when the socket is contained, the periodontal phenotype is forgiving, the implant can be positioned correctly, and the endodontic/infectious story is fully under control. A missing buccal wall is no longer an absolute “never” as a recent randomized controlled trial in the Journal of Periodontology suggests that carefully augmented defect sites can still do well, but it is not a routine immediate case. Thin tissue, midfacial recession, incisive-canal constraints, or active periapical disease at the site or adjacent to it still push us toward staged therapy, because in the esthetic zone, “not yet” can be the most esthetic answer.